Don’t take breaks from supplements? In some cases, you may be doing yourself harm.
Not every supplement should be taken every day indefinitely. In many cases, a cycle, a break, and a clear reassessment work better.

Table of contents
Introduction
Supplementation can easily shift from a targeted tool into an automatic habit. At first, there is usually a clear reason: a deficiency, stress, poor sleep, weaker recovery, an unfavorable lipid profile, gut issues, or a period of more intense training. After a few weeks, however, the supplement often becomes a fixed part of the day — just like brushing your teeth or drinking morning coffee. The problem is that not every supplement is suitable for indefinite daily use.
This does not mean that supplements are inherently dangerous. In many situations, they can be useful and practical. The point is rather that some of them work more like temporary interventions than basic nutrients. Zinc, selenium, ashwagandha, berberine, bergamot, probiotics, and high-dose vitamin C often make the most sense when they address a specific problem, are used at an appropriate dose, and are reassessed after a defined period.
The most practical approach can be summarized as: cycle → measure or observe → decide. Instead of assuming that something should be taken all year round, it is better to define the goal, duration, and stopping criteria. This turns supplementation into a tool that supports health rather than another layer of longevity overkill.
This article is not medical advice, diagnosis, or treatment. If you have a medical condition, take medication, have abnormal blood test results, are pregnant, or have liver, kidney, or immune system issues, supplementation decisions should be discussed with a qualified professional.
Example
Nolan is 38, strength trains three times per week, does zone 2 cardio, and has been interested in longevity for several years. His supplementation started reasonably: magnesium for sleep, creatine for training, omega-3, and vitamin D after checking his 25(OH)D level. Then more products were added: zinc “for immunity”, selenium “for thyroid support”, ashwagandha “for stress”, berberine “for glucose”, a probiotic “for the gut”, glutathione “for mitochondria”, and vitamin C “for oxidative stress”.
After a few months, Nolan realized he was taking more than a dozen capsules per day, but he could not clearly say which ones were actually helping. He did not know whether zinc had improved his immune resilience or was slowly lowering his copper status. He did not know whether berberine was necessary, given that his glucose was already stable. He did not know whether the probiotic was helping his gut or simply causing more bloating. Supplementation had become more of a control ritual than a precise tool.
A more reasonable model would look different. Nolan could keep the fundamentals that have a clear purpose and good tolerance, while organizing the rest into cycles. For example: 8 weeks of ashwagandha during a higher-stress period, then a break and an assessment of sleep, tension, and recovery. 12 weeks of bergamot, then lipid panel and ApoB. 8 weeks of a probiotic, then an honest review of digestive symptoms. In this approach, supplementation stops being a list of things taken “just in case” and becomes a decision system.
Why supplements should not run on autopilot
The biggest issue with supplementation is not always that people take too much of one substance. More often, the problem is a lack of a clear reason, a lack of measurement, and a lack of a defined moment when you can say: “this works”, “this does not work”, or “this is no longer needed”. In practice, many people take supplements for longer than the studies that originally made those interventions interesting.
It helps to distinguish between three types of supplements. The first group includes foundational nutrients or compounds that fill a dietary gap or support a repeated physiological process, such as vitamin D when levels are low, creatine for training, omega-3 when fatty fish intake is low, or magnesium when intake is insufficient or demand is higher. The second group includes targeted interventions intended to influence a specific issue, such as lipids, glucose, stress, sleep, or gut symptoms. The third group includes substances with a narrower safety window or a potential to disturb the balance of other nutrients.
The second and third groups are the ones that most often require a cyclical approach. The reason is simple: the more a supplement behaves like an intervention, the more it should have a goal, a duration, and a reassessment point.
Before starting or continuing a supplement, it is worth asking a few practical questions:
- Do I know what specific problem I am trying to solve, or am I taking this supplement because it “might be useful”?
- Do I have a marker, symptom, or measurable parameter that will allow me to assess the effect after a few weeks?
- Do I know the potential risk of long-term use, especially at a higher dose?
- Could this supplement interact with medication, other supplements, or disturb the status of other nutrients?
- If I stop taking it, will I be able to see whether anything actually gets worse?
This is not an anti-supplement stance. It is an attempt to move supplementation away from “more is better” and toward intentional management of inputs.
Supplements that are most often worth cycling
Some supplements are particularly well suited to a phased model because long-term use may increase the risk of side effects, disturb the balance of other nutrients, or simply lack a good rationale without a specific goal.
Zinc
Zinc is important for immune function, metabolism, skin, hormonal health, and many enzymes. That does not mean that high-dose zinc should be taken indefinitely. Especially at doses around 25–50 mg per day, zinc is better treated as a course rather than a permanent supplement.
The key risk is impaired copper status. Long-term high zinc intake can reduce copper absorption, which in severe cases may contribute to anemia, neurological symptoms, paresthesia, weakness, and gait problems. This is a good example of a supplement that may support one area while gradually creating a problem in another.
A practical model is 6–12 weeks of use, followed by a break and, when appropriate, testing: zinc, copper, ceruloplasmin, and complete blood count. Lower doses, such as 10–15 mg per day, may be more suitable for longer use, but diet and other multivitamin formulas should still be considered.
Selenium
Selenium has a narrower safety window than many people assume. Deficiency can be a problem, but excess can be a problem too. This is especially relevant when someone combines a selenium supplement with fortified products and foods naturally rich in selenium.
Too much selenium may be associated with symptoms such as brittle hair and nails, a metallic taste, garlic-like breath odor, nausea, diarrhea, fatigue, and irritability. With substantial long-term excess, neurological symptoms may also occur. This is why selenium should rarely be treated as a “forever” supplement unless there is a clear reason and appropriate monitoring.
In practice, a reasonable model is 8–12 weeks or 3 months of supplementation, followed by a 3-month break. Even better, the decision should be based on testing and total dietary intake. Selenium is not a supplement where dose improvisation is a good idea.
Ashwagandha
Ashwagandha is often seen as a gentle adaptogen, but in practice it is an herbal intervention that may influence stress, tension, sleep, and subjective well-being. It is not a nutrient that the body requires daily in the same way as protein, magnesium, or vitamin D.
It is most reasonable to use ashwagandha during periods of higher psychological load, poorer sleep, or elevated tension. A typical model is 6–8 weeks of use, followed by a 2–4 week break and reassessment. It is worth paying attention not only to improved sleep or calmness, but also to possible side effects such as sleepiness, reduced drive, digestive symptoms, or unusual liver-related symptoms.
With longer use, it may be worth checking ALT, AST, ALP, and bilirubin. Extra caution is needed in people with liver disease, thyroid disorders, autoimmune conditions, or those taking sedative medications.
High-dose vitamin C
Vitamin C from food and high-dose vitamin C supplementation are not the same thing. Vegetables and fruits provide vitamin C together with fiber, polyphenols, and other bioactive compounds. Taking 1–2 g of supplemental vitamin C per day without a specific reason is a different type of intervention.
High doses may cause diarrhea, gastrointestinal discomfort, heartburn, and in some people may potentially increase the risk of kidney stones. People with a history of kidney stones, kidney issues, or high susceptibility to gastrointestinal symptoms should be especially cautious.
In practice, high-dose vitamin C is better used periodically: during an infection, a phase of higher physical or psychological load, a short period of increased oxidative stress, or a specific clinical indication. For everyday use, a diet rich in vegetables and fruits is the more reasonable foundation.
Supplements that depend on markers and a specific goal
The second group of supplements is not necessarily “dangerous” when used longer term, but its usefulness depends on whether the supplement is solving a specific problem. Without measurement, it is easy to fall into a trap: the supplement is taken for months, but nobody knows whether it is actually improving anything.
Berberine
Berberine is one of the substances that often enters the longevity world because it is associated with glucose, insulin, lipids, and metabolic health. The problem is that in a metabolically healthy person, with stable glucose and no clear signs of impaired insulin sensitivity, constant berberine use may simply be unnecessary.
It is more of a metabolic intervention than a basic supplement. It makes the most sense when there is a specific goal: elevated fasting glucose, impaired insulin sensitivity, an unfavorable lipid profile, increased body fat, or a defined dietary experiment. In that case, it can be used for 8–12 weeks, followed by glucose, insulin, HOMA-IR, lipid panel, and liver enzyme assessment.
Potential issues include gastrointestinal symptoms and interactions with medications, especially glucose-lowering, anticoagulant, or metabolism-related drugs. Berberine should not be treated as “metabolic insurance” when markers are already excellent.
Bergamot
Bergamot makes the most sense as a lipid-focused intervention. If the goal is to lower LDL-C, non-HDL-C, or ApoB, it can be used as part of a test protocol. Without a lipid panel and ApoB, however, its use is imprecise.
The most practical model is testing before starting, 8–12 weeks of supplementation, and then repeating the lipid panel and ApoB. If the effect is clear, continuation or another cycle may be considered. If there is no effect, ongoing use makes little sense.
The main risk is usually not acute toxicity, but a false sense of control. Someone may take bergamot for a year while ApoB remains too high. A supplement should not replace measurement.
Probiotics
Probiotics are one of the most overused supplement categories. They are often marketed as something that “rebuilds the microbiome”, but in practice their effects are strain-specific, temporary, and context-dependent. One probiotic may make sense after antibiotics, another for diarrhea, another for IBS, and another for specific digestive symptoms.
Taking a random probiotic all year round is rarely the best strategy. A better model is 4–12 weeks, symptom tracking, and reassessment. If there is no improvement in digestion, bowel movement regularity, bloating, or food tolerance after several weeks, it may be better to change the strain, change the strategy, or take a break.
In most healthy people, probiotics are well tolerated, but they may cause bloating, discomfort, and changes in bowel rhythm. In people who are severely ill, immunocompromised, have catheters, or recently underwent major medical procedures, the decision should be especially cautious.
Saffron
Saffron can be an interesting tool for mood, tension, appetite, compulsive snacking, or subjective stress. That does not mean it should be taken indefinitely.
It is best treated as a 6–8 week experiment. Before starting, it is worth defining what should improve: mood, sleep, appetite, stress, snacking, or focus. After the cycle, the effect should be assessed honestly. If there is no noticeable benefit, continuing is likely just adding another capsule rather than building a real strategy.
Potential side effects are usually mild, but may include gastrointestinal symptoms, sleepiness, headaches, or appetite changes. The key limitation is the lack of strong long-term data for indefinite use in healthy people.
Glutathione
Glutathione is often used for antioxidant support, mitochondrial support, or recovery. It may make sense in a specific context, but it is also a good example of a supplement that should be assessed pragmatically: is the effect noticeable, measurable, and worth the cost?
A model of 8–12 weeks or 3–6 months may be reasonable if there is a clear goal. After that period, it is worth taking a break and checking whether anything has actually changed: energy, recovery, HRV, training tolerance, inflammatory markers, liver enzymes, or other context-specific parameters.
If stopping it makes no difference, and there was no clear improvement during use, the supplement may not be worth continuing. It is also worth remembering that the body produces glutathione endogenously, and foundations such as sleep, adequate protein intake, recovery, vegetables, and training load management may matter more than the capsule itself.
Supplements that can usually be used longer term
Not all supplements require cycling. Some can be used long term if there is a clear reason, good tolerance, and periodic reassessment. This distinction matters because the goal is not to take breaks from everything, but to separate foundations from interventions.
This group often includes:
- Creatine, especially in people who strength train, practice intensive sport, or want to support muscle mass. When well tolerated, it usually does not require cycling, although hydration, digestive comfort, and bloodwork should still be interpreted in the broader health context.
- Omega-3, especially if the diet contains little fatty fish or the goal is to improve the omega-3 index, inflammatory balance, or cardiovascular support. Here, dose and product quality matter more than cycling.
- Vitamin D, when 25(OH)D levels indicate supplementation. The key is not cycling, but adjusting the dose to the result, season, sun exposure, and body weight.
- Magnesium, especially with low dietary intake, high stress, intense training, or poorer sleep. The key considerations are gastrointestinal tolerance and the form of magnesium used.
- Fiber, if it is well tolerated and supports bowel regularity, glucose control, satiety, and the microbiome. Here, gradual dose increases and adequate hydration matter more than breaks.
- Protein powder, if it helps meet daily protein needs. It is more of a functional food than a classic supplement, though digestive tolerance and ingredient quality still matter.
Even in this group, periodic review is useful. A long-term supplement should still have a reason. The difference is that breaks are usually less important here than they are with zinc, selenium, ashwagandha, berberine, or high-dose vitamin C.
How to approach breaks in practice
The simplest system is to divide supplements into three categories: stable foundations, targeted cycles, and experimental supplements. This makes it easier to avoid chaos and determine what is actually working.
Stable foundations are supplements with a clear reason and relatively low risk when used appropriately. Targeted cycles are supplements used for a defined period, such as 8–12 weeks. Experimental supplements are those whose effect is uncertain and requires especially honest evaluation.
A practical framework can look like this:
- Before starting a cycle, write down the goal of the supplement, such as improved ApoB, better sleep, less bloating, lower stress, more stable glucose, or improved recovery.
- Define the duration, most often 6–12 weeks, depending on the supplement and goal.
- Avoid adding several new supplements at once if you want to know which one is working.
- After the cycle, assess the effect using markers, symptoms, or data from devices, such as HRV, sleep, glucose, or training tolerance.
- If the effect is unclear, take a break and observe whether anything worsens after stopping.
- If there is no effect, do not continue just because the supplement “should theoretically help”.
The most practical principle is: a supplement without a goal should be questioned. It does not always need to be stopped immediately, but you should know why it is in the plan.
Common mistakes
In longevity supplementation, the biggest mistakes often do not come from ignorance, but from overenthusiasm. The more someone cares about health, the easier it is to believe that another intervention will add another few percent of advantage. The problem is that the body is not a spreadsheet where every added supplement creates a separate, predictable bonus.
The most common mistakes include:
- Taking supplements without an endpoint. If you do not know when to stop, you probably do not have a clearly defined goal.
- Adding several things at once. If sleep, digestion, or energy improves, you will not know what helped. If side effects appear, it will also be harder to identify the cause.
- Confusing short-term benefit with long-term necessity. Something that helps for 6 weeks during a stressful period does not necessarily need to be taken all year.
- Ignoring interactions. Berberine, ashwagandha, zinc, selenium, and high-dose vitamin C may matter in combination with medications, other supplements, or specific health issues.
- Replacing markers with hope. For lipids, glucose, mineral status, or liver function, subjective feelings are not enough. Measurement matters.
- Supplementing anxiety. Sometimes supplements do not solve a health problem; they create a sense of control. In that case, reducing the list may be more useful than expanding it.
In practice, a good supplement plan should be shorter, more intentional, and easier to evaluate. The number of capsules does not define the quality of a protocol. Alignment with the body’s actual needs does.
How to easily manage supplement cycles and schedules
In practice, the biggest challenge is not simply determining that a given supplement is worth using cyclically. The harder part is keeping track of the schedule afterward: when to start the cycle, when to take a break, when to return to supplementation, and when to reassess the effects. With several or even a dozen supplements, it is very easy to lose the rhythm, especially if some are used continuously, some temporarily, and some cyclically.
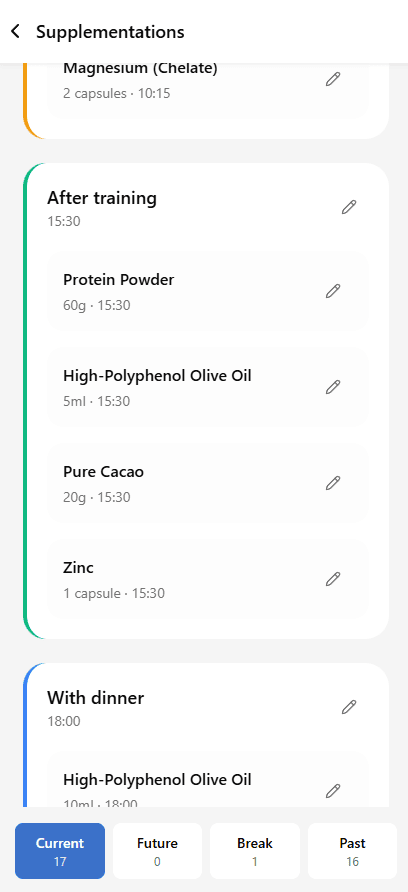
In the free Longevity Protocols mobile app, you can organize supplementation in a more systematic way. The app allows you to add supplements to specific times of day, assign intake times, edit doses, and arrange them into clear groups, such as after training or with dinner. As a result, supplementation is not just a loose list of products, but becomes a practical daily schedule.
The app supports different types of supplementation, which fits well with the approach described in this article:
- Continuous supplements can be set for ingredients that make sense long term, for example when they result from diet, lifestyle, training, or regularly monitored markers.
- Temporary supplements can be planned as a short intervention for a specific period, for example a few weeks of support during higher stress, travel, infection, or a dietary change.
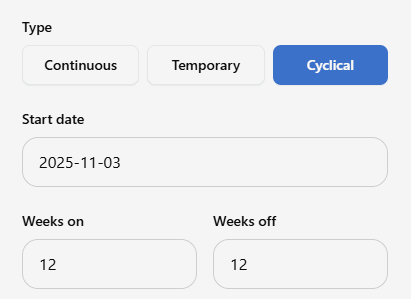
- Cyclical supplements can be scheduled in a “weeks on / weeks off” model, for example 12 weeks of use and 12 weeks of break. This is especially useful for supplements such as zinc, selenium, ashwagandha, berberine, bergamot, or other interventions that are worth reassessing periodically.
In practice, you can therefore set not only the supplement name and dose, but also the start date, the number of weeks on, and the number of weeks off. This helps you plan the entire cycle in advance, instead of remembering it manually or maintaining a separate spreadsheet.
On a daily basis, the app shows supplements in a clear breakdown by statuses such as current, future, break, and past. This allows you to immediately see which supplements are currently being used, which will start in the future, which are on a break, and which already belong to completed interventions. This is especially important if you want to treat supplementation as an organized protocol rather than a set of random decisions.
A major advantage of such a system is reminders. The app can notify you about the start of a cycle, the end of a cycle, or an upcoming change in supplement status. In the notifications panel, you can see how many reminders are left and then go to the details. This means you do not have to remember everything yourself — if a supplement is supposed to return after a break or should be ended after a specific number of weeks, the app helps you not miss that moment.
Additionally, Longevity Protocols can also send email notifications about supplements. This is useful as a second layer of reminders, especially when cycles are longer, there are more supplements, or you want to avoid missing the moment of review, break, or restarting supplementation.
This is exactly the kind of approach that best fits conscious supplementation: not only “what to take”, but also when to start, when to stop, when to check the effects, and when to make the next decision.
You can learn more about the Longevity Protocols app here:
https://longevity-protocols.com/en/app/
Summary
Supplements do not all need to follow the same model. Some can make sense long term if they address a stable need, are well tolerated, and are periodically reviewed. Others are better treated as cyclical interventions, especially when they affect metabolism, the nervous system, the microbiome, mineral status, or have a narrower safety window.
The supplements that are most often worth cycling include higher-dose zinc, selenium, ashwagandha, berberine, bergamot, probiotics, and high-dose vitamin C. Saffron, glutathione, and CoQ10 can often be treated more as test-based or optional cycles. Supplements that usually require less cycling include creatine, omega-3, magnesium, fiber, vitamin D adjusted to blood levels, and protein powder used to meet dietary protein needs.
The best practical recommendation is: 8–12 weeks of use, a marker or clear observation before and after, then a decision. If a supplement has no goal, produces no effect, or you do not know what it is supposed to improve, it is worth putting aside. Longevity is not about doing as much as possible. It is about doing the right things, at the right time, for the right reason.
Bibliography
-
NIH Office of Dietary Supplements. Copper – Health Professional Fact Sheet.
https://ods.od.nih.gov/factsheets/Copper-HealthProfessional/ -
Pabla P, et al. Zinc-Induced Copper Deficiency as a Rare Cause of Neurological Deficit and Anemia.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10510946/ -
EFSA Panel on Nutrition, Novel Foods and Food Allergens. Scientific opinion on the tolerable upper intake level for selenium.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9854220/ -
NIH Office of Dietary Supplements. Zinc – Health Professional Fact Sheet.
https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/ -
Philips CA, et al. Ashwagandha-induced liver injury — A case series from India and literature review.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10531359/ -
Philips CA, et al. Ashwagandha-induced liver injury — A case series from India and literature review. PubMed.
https://pubmed.ncbi.nlm.nih.gov/37756041/ -
Kell G, et al. Effects of saffron extract supplementation on mood, well-being, and response to a psychosocial stressor in healthy adults.
https://pmc.ncbi.nlm.nih.gov/articles/PMC7882499/ -
Health Science Reports. Adverse events of saffron (Crocus sativus L.): Systematic review.
https://onlinelibrary.wiley.com/doi/full/10.1002/hsr2.72212 -
Efficacy and safety of berberine on the components of metabolic syndrome: A systematic review and meta-analysis.
https://pmc.ncbi.nlm.nih.gov/articles/PMC12307485/ -
Efficacy and safety profile of berberine treatment in metabolic and cardiovascular health.
https://mednexus.org/doi/10.1097/CD9.0000000000000087 -
The effect of bergamot supplementation on lipid profile: A systematic review and meta-analysis.
https://onlinelibrary.wiley.com/doi/10.1002/ptr.7647 -
Mollace V, et al. Effects of 12-week supplementation of Citrus bergamia extracts on cardiometabolic risk factors.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5741859/ -
Frontiers in Nutrition. A narrative review on the use of probiotics in several clinical conditions.
https://www.frontiersin.org/journals/nutrition/articles/10.3389/fnut.2023.1209238/full -
Besselink MG, et al. Infectious complications following probiotic ingestion: A systematic review.
https://link.springer.com/article/10.1186/s12906-018-2394-3 -
Richie JP, et al. Randomized controlled trial of oral glutathione supplementation on body stores of glutathione.
https://pubmed.ncbi.nlm.nih.gov/24791752/ -
Richie JP, et al. Randomized controlled trial of oral glutathione supplementation on body stores of glutathione. ResearchGate version.
https://www.researchgate.net/publication/262050454_Randomized_controlled_trial_of_oral_glutathione_supplementation_on_body_stores_of_glutathione -
NIH Office of Dietary Supplements. Vitamin C – Health Professional Fact Sheet.
https://ods.od.nih.gov/factsheets/VitaminC-HealthProfessional/ -
Thomas LDK, et al. Ascorbic acid supplements and kidney stone incidence among men: A prospective study.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/1568519 -
Ferraro PM, et al. Total, dietary, and supplemental vitamin C intake and risk of incident kidney stones.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4769668/
